

Published in:
Abstract
BACKGROUND Guidelines recommend a trial of one or more antiarrhythmic drugs before catheter ablation is considered in patients with atrial fibrillation. However, first-line ablation may be more effective in maintaining sinus rhythm.
METHODS We randomly assigned 303 patients with symptomatic, paroxysmal, untreated atrial fibrillation to undergo catheter ablation with a cryothermy balloon or to receive antiarrhythmic drug therapy for initial rhythm control. All the patients received an implantable cardiac monitoring device to detect atrial tachyarrhythmia. The follow-up period was 12 months. The primary end point was the first documented recurrence of any atrial tachyarrhythmia (atrial fibrillation, atrial flutter, or atrial tachycardia) between 91 and 365 days after catheter ablation or the initiation of an antiarrhythmic drug. The secondary end points included freedom from symptomatic arrhythmia, the atrial fibrillation burden, and quality of life.
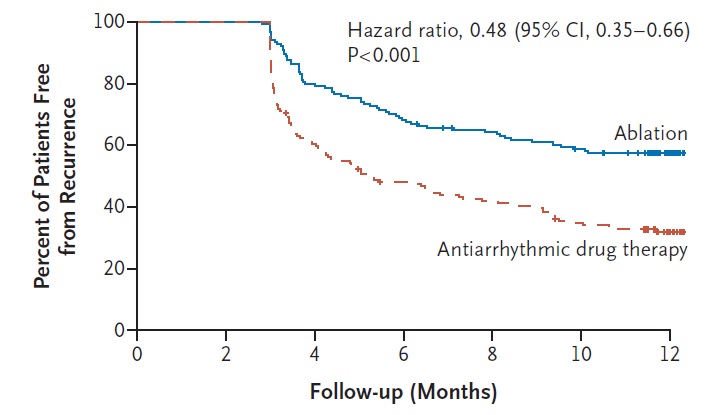
RESULTS At 1 year, a recurrence of atrial tachyarrhythmia had occurred in 66 of 154 patients (42.9%) assigned to undergo ablation and in 101 of 149 patients (67.8%) assigned to receive antiarrhythmic drugs (hazard ratio, 0.48; 95% confidence interval [CI], 0.35 to 0.66; P<0.001). Symptomatic atrial tachyarrhythmia had recurred in 11.0% of the patients who underwent ablation and in 26.2% of those who received antiarrhythmic drugs (hazard ratio, 0.39; 95% CI, 0.22 to 0.68). The median percentage of time in atrial fibrillation was 0% (interquartile range, 0 to 0.08) with ablation and 0.13% (interquartile range, 0 to 1.60) with antiarrhythmic drugs. Serious adverse events occurred in 5 patients (3.2%) who underwent ablation and in 6 patients (4.0%) who received antiarrhythmic drugs.
CONCLUSIONS Among patients receiving initial treatment for symptomatic, paroxysmal atrial fibrillation, there was a significantly lower rate of atrial fibrillation recurrence with catheter cryoballoon ablation than with antiarrhythmic drug therapy, as assessed by continuous cardiac rhythm monitoring. (Funded by the Cardiac Arrhythmia Network of Canada and others; EARLY-AF ClinicalTrials.gov number, NCT02825979. opens in new tab.)
This randomized trial was presented at the American Heart Association Scientific Sessions and simultaneously published in the New England Journal of Medicine. This study features work by CCI Investigator Dr. Jason Andrade.
The Centre for Cardiovascular Innovation (CCI) is a clinical research operations centre that provides its member cardiovascular investigators with access to dedicated, expert personnel as well as organizational and physical infrastructure that will enhance their research scope and capacity.


